Original link: https://kaopubear.top/blog/2022-12-02-tumor-aneuploidy-predicts-ici-survival/
written in front
The book continues from the previous chapter. In yesterday’s article, we started from the experience of publishing two large sub-journals of Nature in one day. We mentioned that Liam Flinn Spurr of the University of Chicago published an article in Nature Cancer as the first author on November 28. A clinical study found that non-small cell lung cancer with high aneuploidy is more sensitive to radiotherapy combined with immunotherapy . At the same time, an article in Nature Genetics online introduced that in patients with low TMB, the degree of tumor aneuploidy can predict the efficacy of pan-cancer immunotherapy .
If you want to see more details of this Nature Cancer article and a short introduction about tumor aneuploidy, you can read yesterday’s article .
In the first half of today’s article, let us continue to look at the content of the second paper published on Nature Genetics. In the second half, we will also pay attention to whether its Peer Review revealed any details behind the reception.
Without further ado, let’s start with the formal content.
Is TMB a good biomarker?
Immunotherapy has revolutionized the way many patients with advanced cancer are treated, but immune checkpoint inhibitors (ICIs) are ineffective for most patients.
In order to find those who can really benefit from ICI treatment, we have been exploring biomarkers that can predict the efficacy of immunotherapy. At present, including PD-L1 expression, CD8 + T cell characteristics, tumor neoantigen burden and TMB have all proved their value in this regard in some studies.
Among them, TMB has been identified as a pan-cancer prognostic and predictive biomarker in ICI therapy in multiple independent studies. For example, an article published by Samstein et al. in Nature Genetics in 2019 analyzed the data of 1662 pan-cancer patients who received ICI treatment and found that the top 20% TMB was related to overall survival. As shown in the figure below, the OS of the top10% TMB patients is better than 10-20%, and the OS of the remaining 80% patients is the worst.
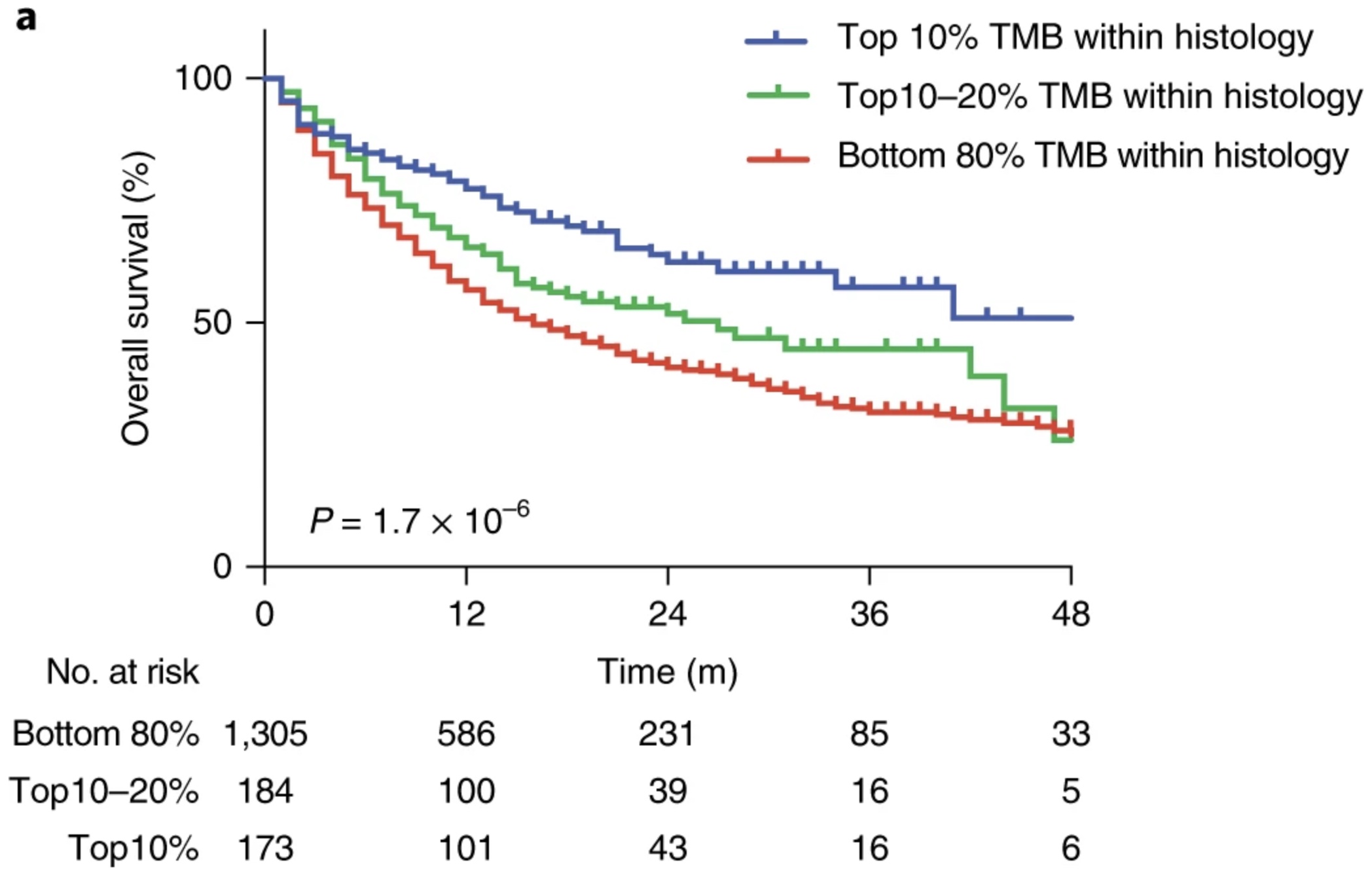
Later, the FDA approved the application of pembrolizumab in pan-cancer, and its high TMB standard was defined as not less than 10 mutations per megabase. From this perspective, there is nothing wrong with TMB as a biomarker for immunotherapy, and it once gave us great hope.
However, let’s not talk about the subsequent doubts about whether TMB is useful in ICI combination, and the debate on what is more appropriate for TMB to set the cutoff. As far as TMB is concerned as a biomarker, we should also see its two sides.
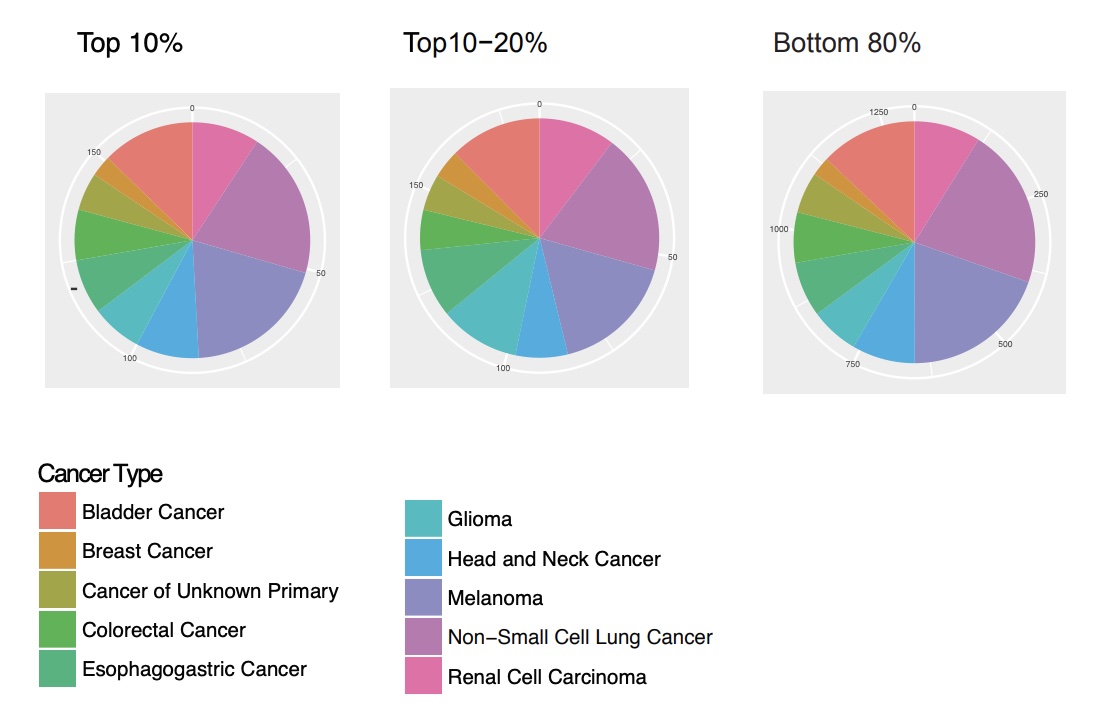
Still the study mentioned above, from the following two figures, we can see the OS HR and TMB cutoff corresponding to each cancer type, as well as the distribution ratio of different cancer types in different gradients of TMB. If 10 is used as the standard of high TMB, the cutoff value of many cancer types in the Cox analysis of this study did not reach 10.
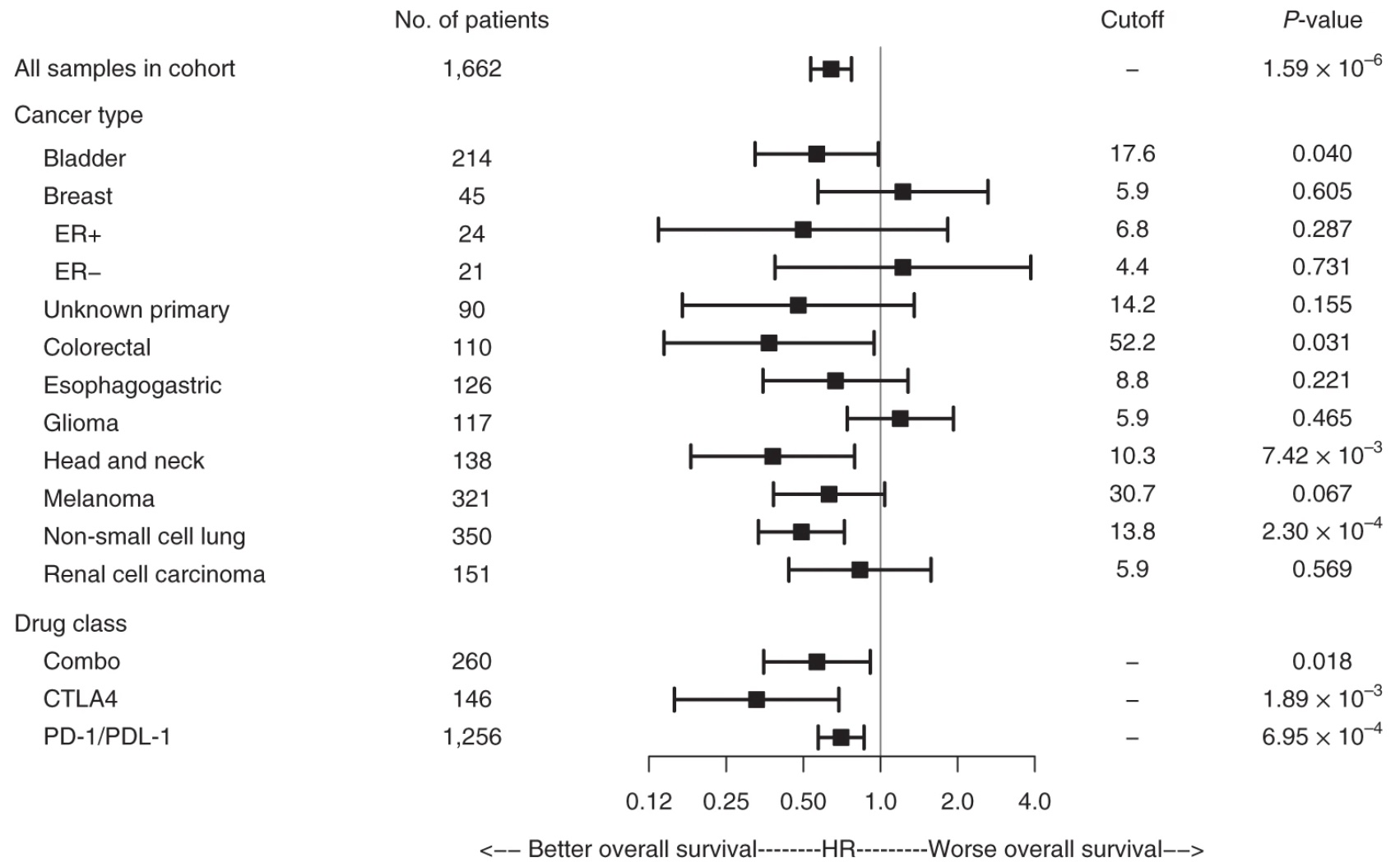
Furthermore, regardless of the threshold used to define high TMB, most patients still exhibit low TMB features, and genomic predictors of outcome in this population are unclear. Therefore, we still need new biomarkers to improve the risk stratification of cancer immunotherapy.
Aneuploidy score distinguishes ICI efficacy
An imbalance in the number of chromosomes or chromosome arms in tumor cells is called aneuploidy, and as mentioned in yesterday’s article, it is an almost universal feature of human cancer. In recent years, different studies have revealed the negative impact of tumor aneuploidy on tumor immunity, and the possible mechanisms include immune evasion, including downregulation of PD-L1 expression and suppression of intratumoral CD8+ T cell responses. In addition, previous studies have demonstrated that a high degree of tumor aneuploidy is actually a marker of poor overall survival and suggested that aneuploidy is suitable as a biomarker of clinical outcome.
In this context, the author’s team of this paper also found that aneuploidy is also an effective biomarker for immunotherapy combined with radiotherapy.
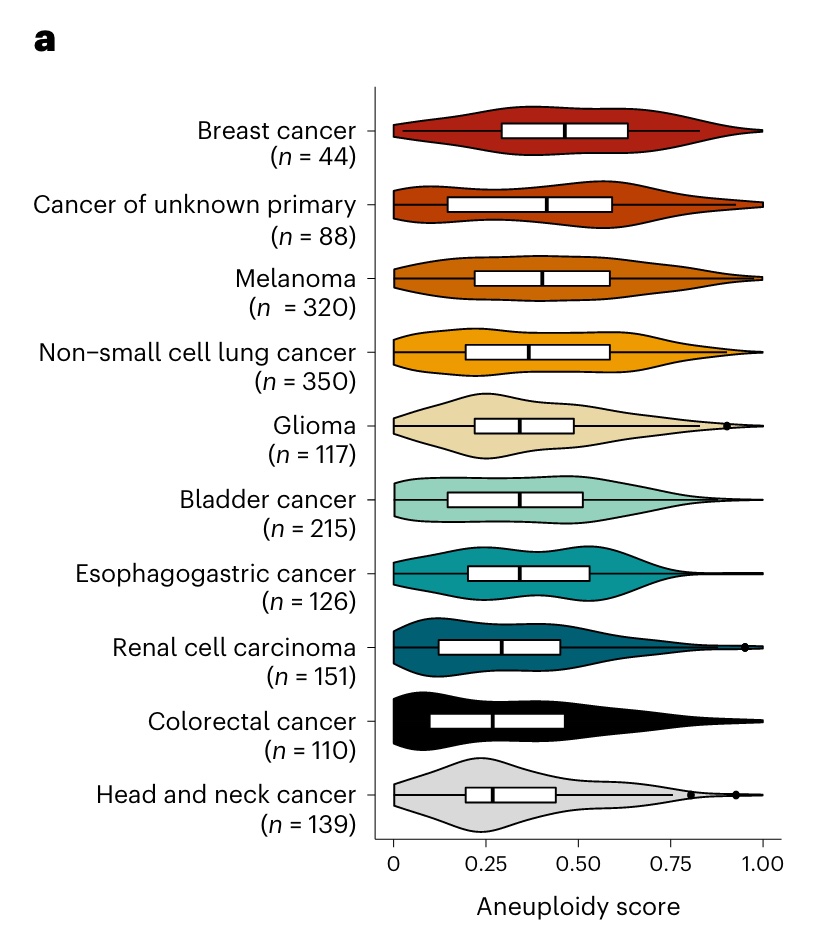
Although aneuploidy is ubiquitous, the degree of aneuploidy varies widely by cancer type. The author’s team reanalyzed the ICI cohort of more than 1,600 patients we mentioned above, and it can be seen that the degree of aneuploidy in breast cancer and melanoma is more obvious overall, while the degree of aneuploidy in renal cell carcinoma, colorectal cancer, and head and neck cancer is more obvious. The degree of euploidy was generally low.
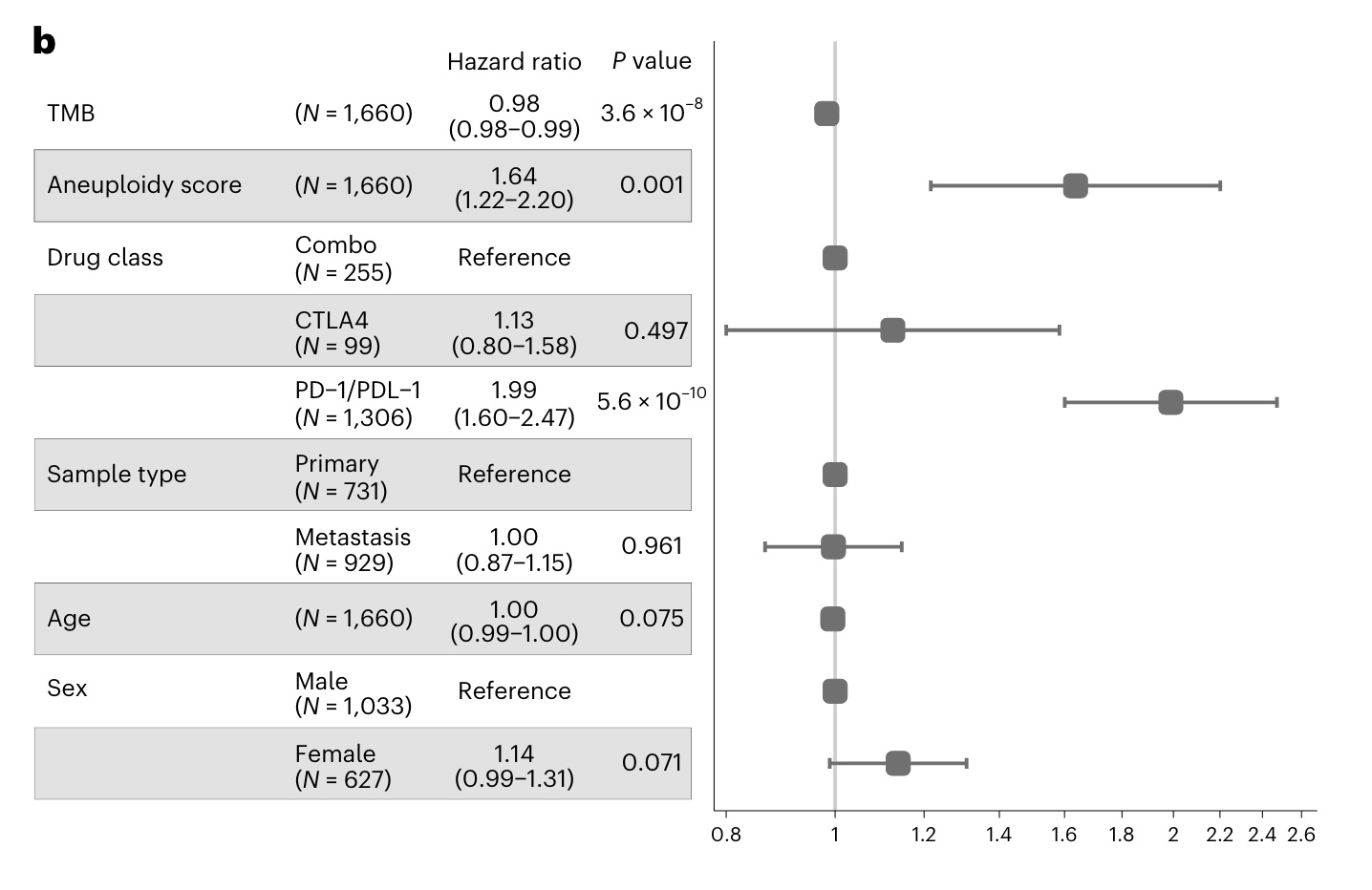
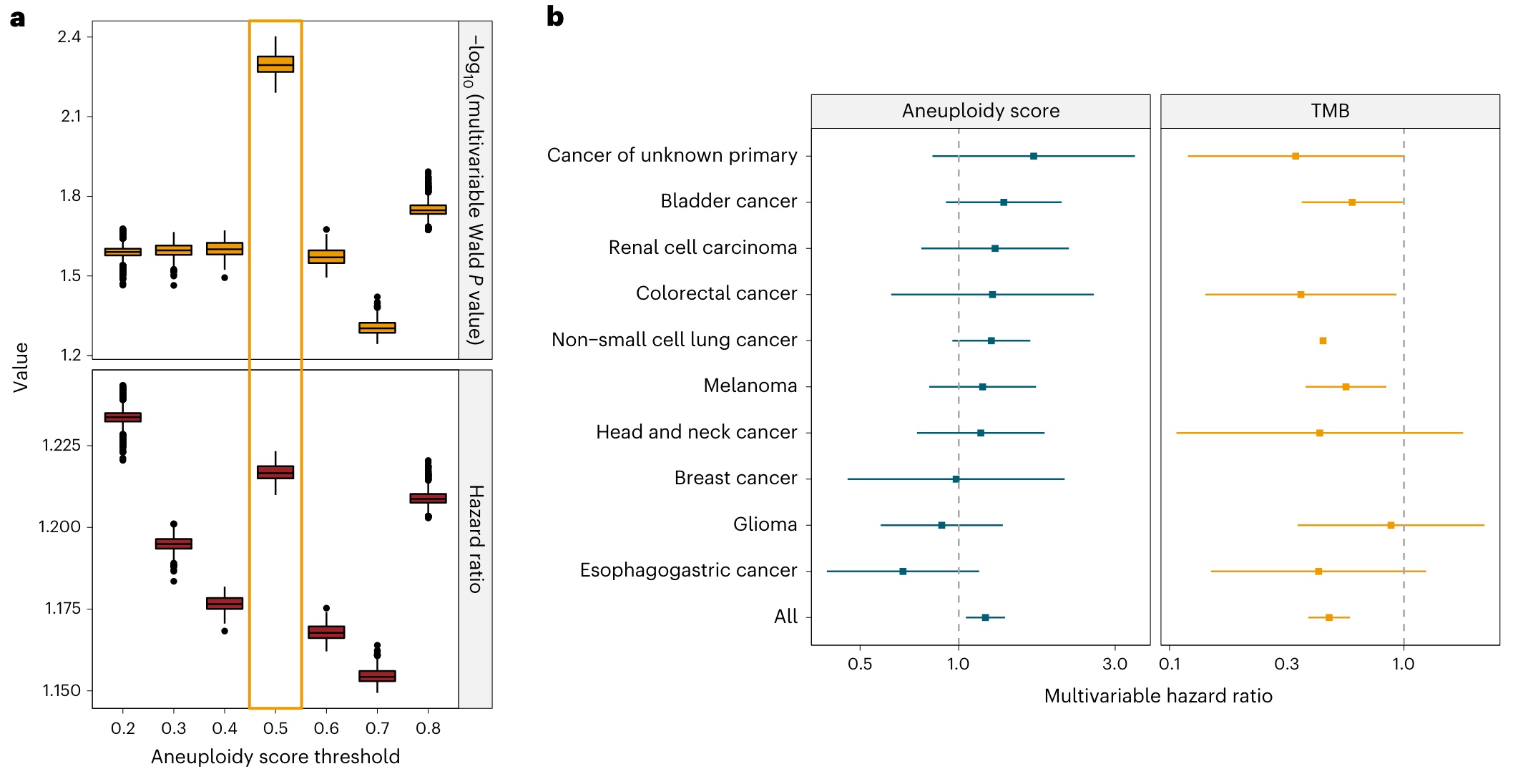
The authors tested the predictive value of aneuploidy score in a multivariate model that included TMB, ICB drug type, and other potential clinical confounders. In all tumors, the results showed that high aneuploidy scores (and both PD-L1) were significantly associated with poor prognosis.
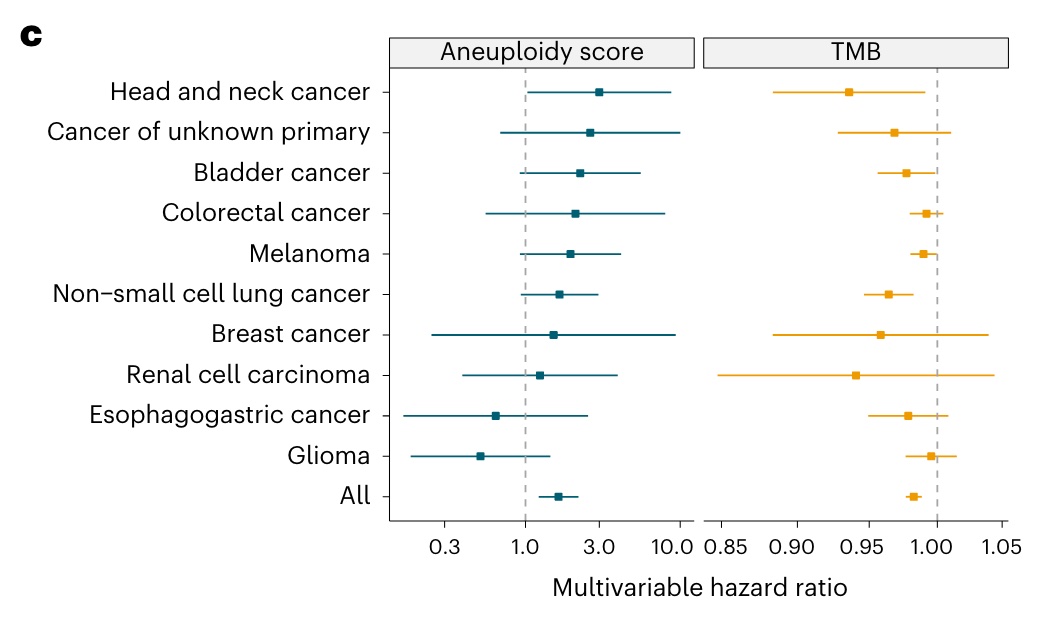
Similar results were observed in most single tumor types.
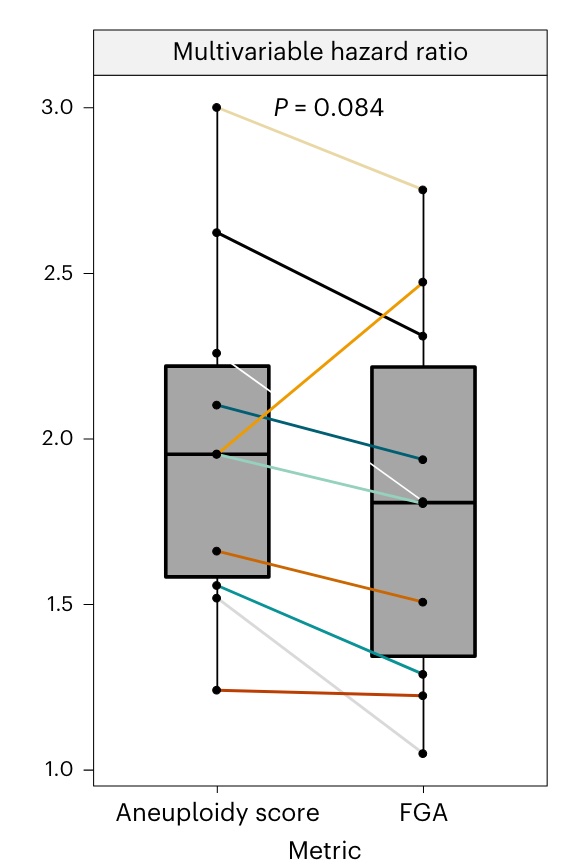
Notably, there was no correlation between TMB and aneuploidy score, also demonstrating the independence of these variables. In addition, another common measure of chromosomal instability is the fraction of genome altered (FGA), which has also been shown to be a marker for predicting tumor immunity.
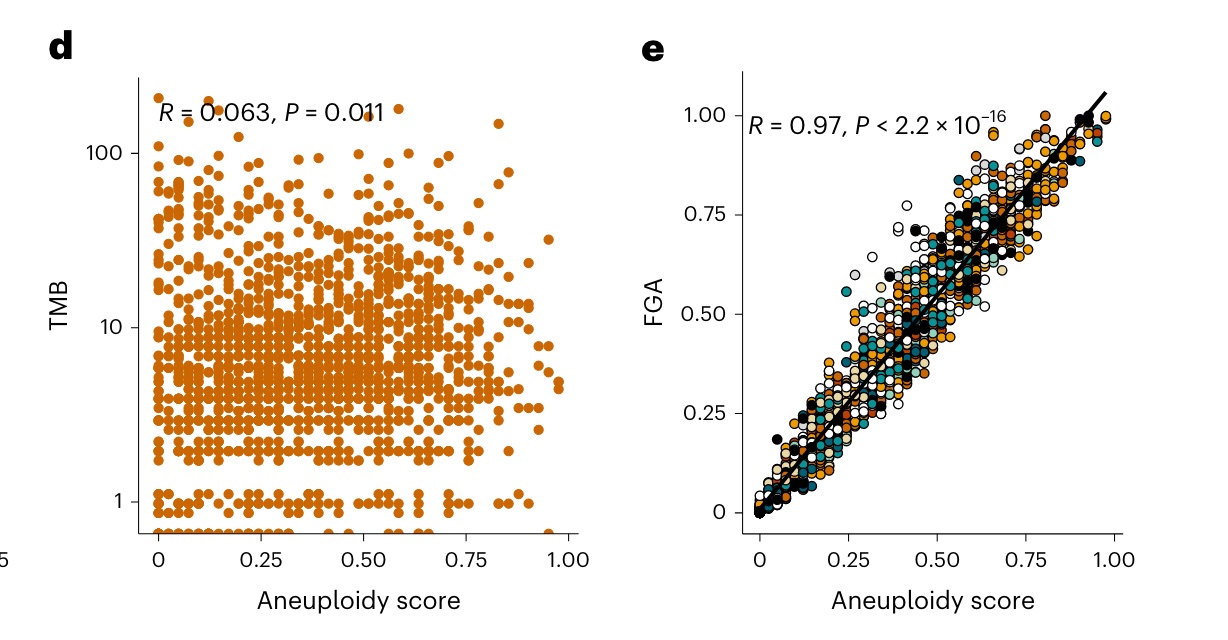
Although it is not difficult to understand that the aneuploidy score and FGA have a high correlation, but by using these two indicators separately for different cancer types to perform multivariate Cox analysis, at least the results of the author’s study in this cohort show that aneuploidy Scores are slightly better.
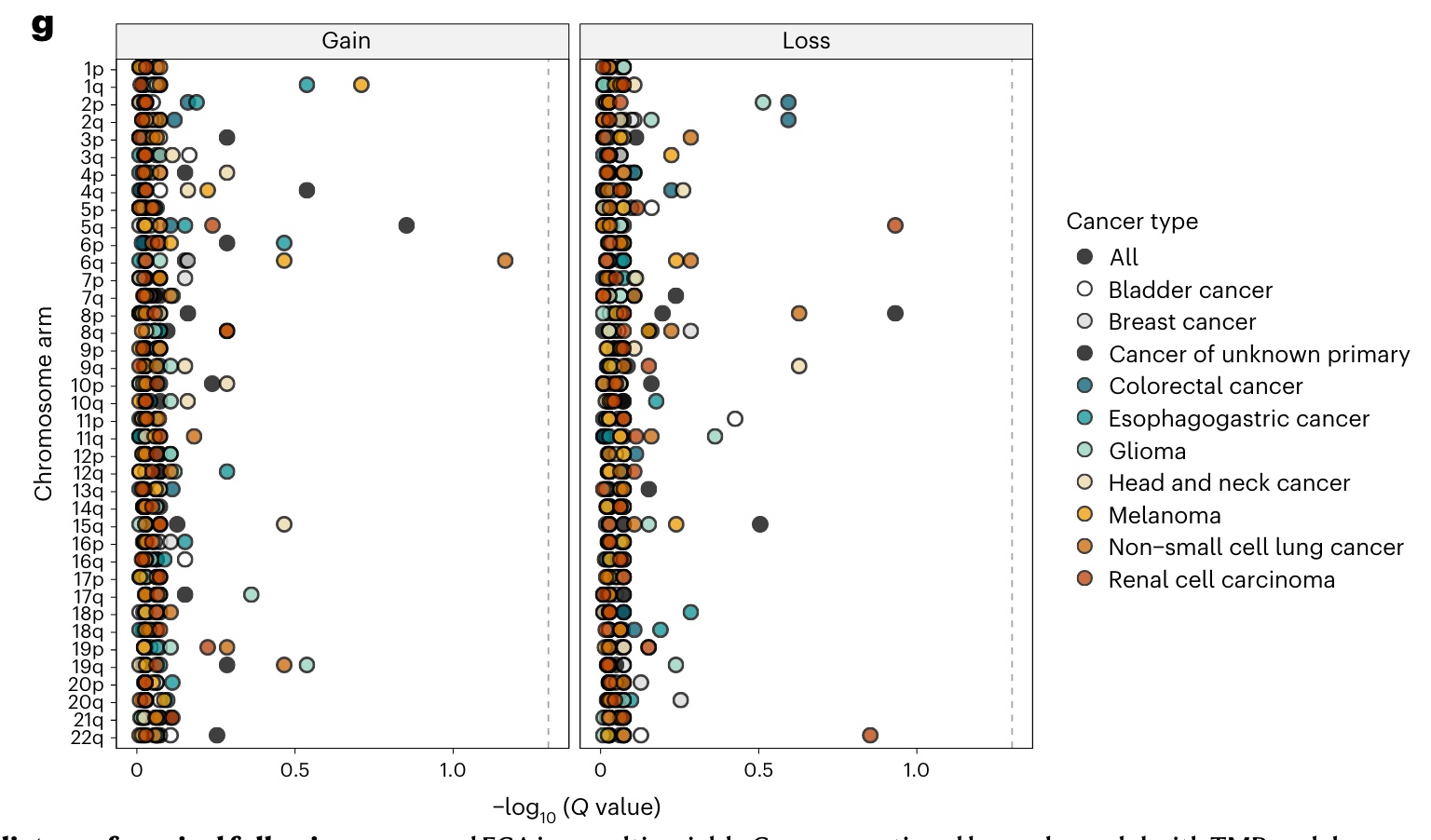
The overall aneuploidy score is composed of the status of each chromosome, so is there a certain chromosome arm that is better for assessing the efficacy of ICI in certain cancers? To answer this question, the authors also examined whether the prognostic value of the aneuploidy score was primarily influenced by specific chromosomal changes (such as loss of heterozygosity at 9p21 in the gene CD274 encoding PD-L1). The results showed that no specific arm-level changes were associated with survival as shown in the figure below when controlling for an FDR of 0.05.
How Aneuploidy Scoring Incorporates TMB
In fact, at this point in the analysis, existing analyzes have supported the use of aneuploidy score as a prognostic biomarker in immunotherapy. However, to facilitate its use as a clinical biomarker, the authors identified an aneuploidy score threshold that best synergized with TMB for risk stratification of ICI-treated patients by using an analysis similar to the TMB threshold above. Simply put, the type of ICI drug is considered in the multivariate model, and the top 20% of TMB is defined as high TMB, and then the aneuploidy score of each tumor type is from 20% to 80%, and each 10% is used as an indicator Perform test analysis. After comparison, it was found that the 50th percentile (top50%) of the aneuploidy score was the best threshold with the lowest p value among all candidate thresholds (as shown in the figure below).
Notably, the same optimal aneuploidy score threshold was also obtained when using the FDA-approved TMB threshold of 10 in the multivariate model.
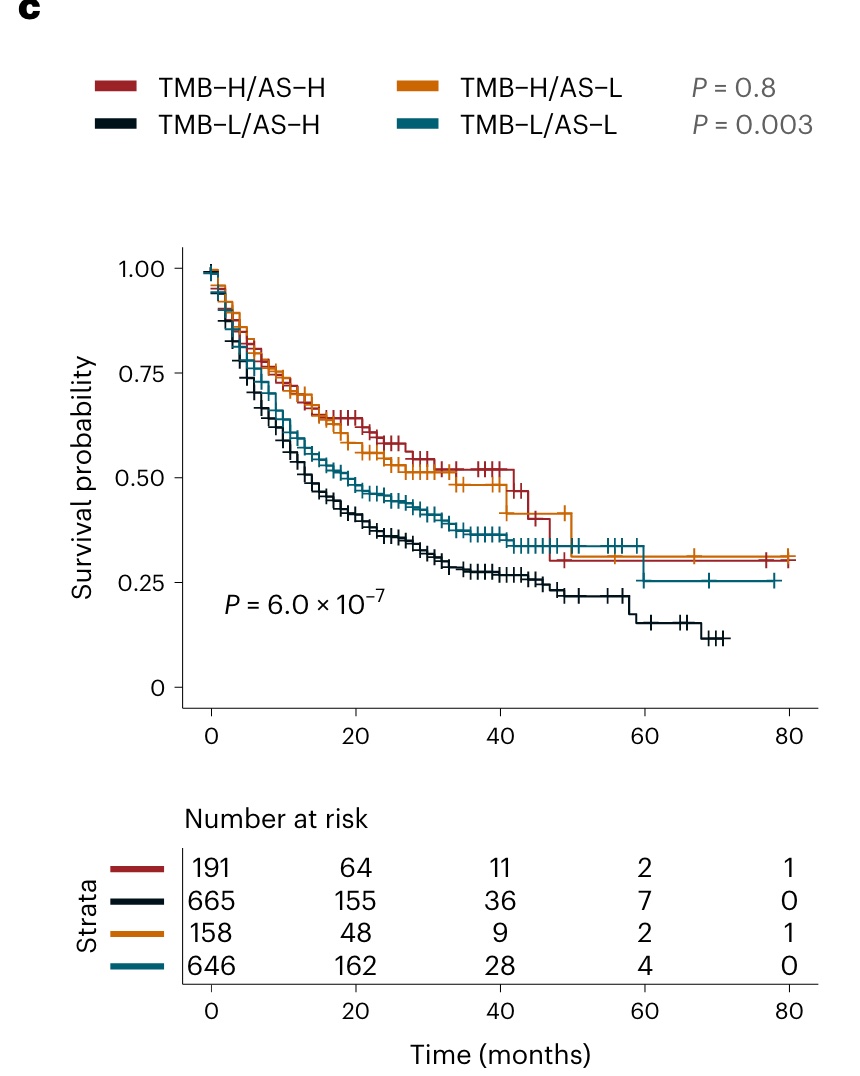
In the KM analysis, using top 20% TMB and top 50% aneuploidy scores as classification criteria, it was concluded that in high TMB tumors, aneuploidy score had no prognostic value; in low TMB tumors, however, more Patients with tumors with high aneuploidy scores had significantly worse prognosis after receiving ICI.
Which cancer types are more affected by aneuploidy score
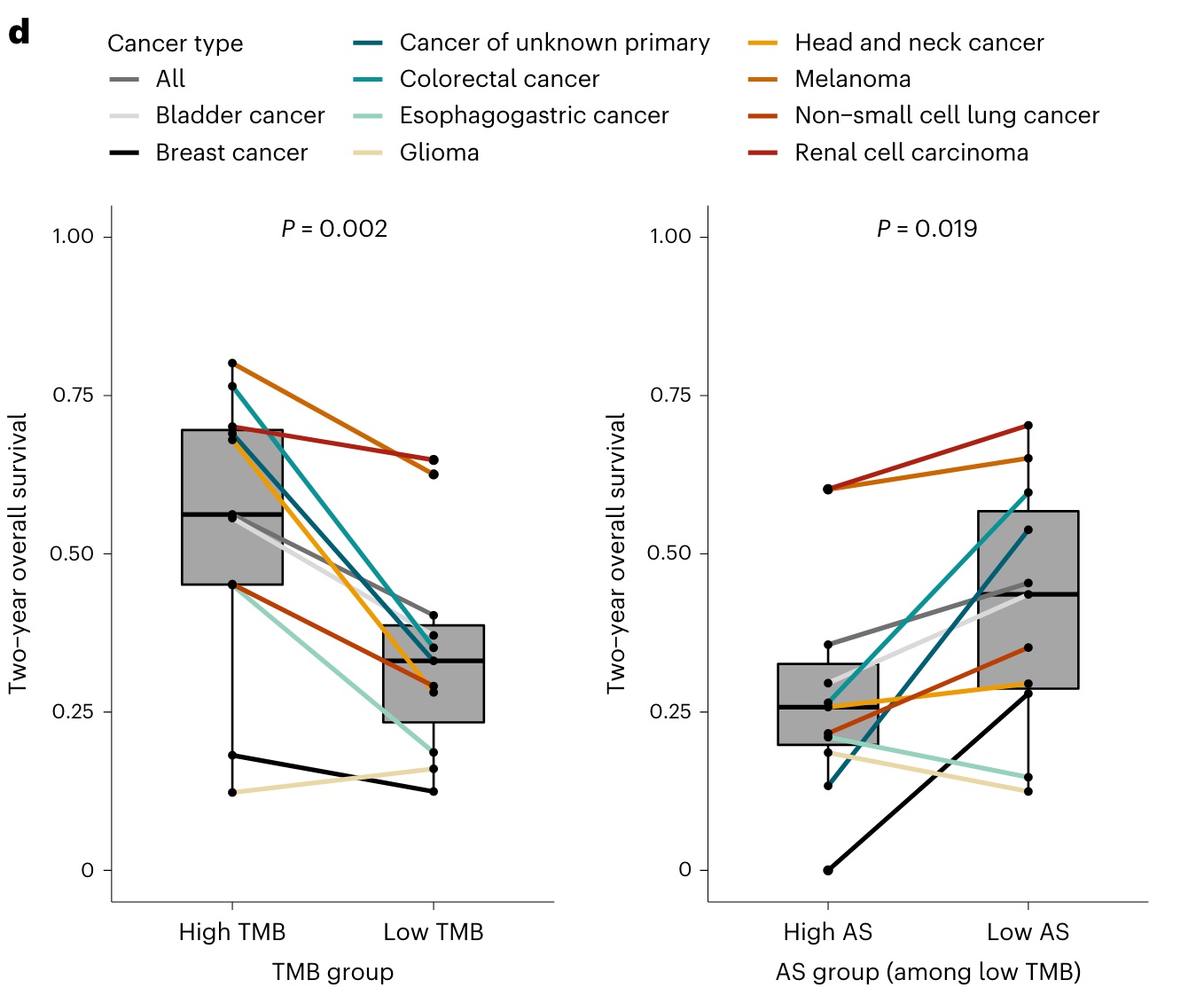
Finally, 2-year OS was compared between different high and low TMB and different high and low aneuploidy scores in different tumor types, respectively. RESULTS: Aneuploidy score had comparable prognostic impact as TMB score in patients with colorectal cancer, bladder cancer, non-small cell lung cancer, and unknown primary location. Aneuploidy scores for breast and kidney cancers showed greater predictive value.
In addition, it is noteworthy that in the low TMB population, the differences in two-year overall survival between patients with high and low aneuploidy scores were greatest for cancers of unknown primary location (13% vs 54%), colorectal cancer (26% vs 60%) and breast cancer (0% vs 28%).
Looking back at this Brief Communication published on Nature Genetics, we can draw the following two conclusions:
1: Elevated aneuploidy score is an independent and complementary predictor of OS in patients with low TMB tumors treated with ICIs.
2: The top 50% aneuploidy score can be used to define a high aneuploidy score threshold, which has an independent prognosis for tumors defined as low TMB under the top20% TMB (or TMB not less than 10 as the standard) classification value.
At the same time, the credibility of this conclusion also requires you to comprehensively consider the number of samples of each cancer type in this data set containing 10 cancer types, as well as some offsets that may be brought about by patient data sets from a single institution. Therefore, if you want to further improve its evidence-based level, prospective clinical research is also essential.
In addition, it is necessary to identify synergistic treatment modalities that may help overcome immune resistance in highly aneuploid tumors in future studies.
Regardless, this multi-cancer retrospective study represents an important step toward gaining insight into the role of tumor aneuploidy in modulating the response to immunotherapy in low-TMB tumors.
what the reviewers said
The magazine has released the detailed documents of Peer Review, let us see what the reviewers say.

First of all, both reviewers spoke highly of the study. As the editor noted, while they did have some requests for improvements, they were relatively simple and didn’t require too much extra work.
And in the final text, what analyzes are the revisions proposed by the reviewers, and what comments do the reviewers have? May wish to guess.
During the review process, the two reviewers mentioned the following four points:
1: The proportion of genome copy number alterations (FGA) is a predictor of tumor immunity, and it is also valuable to discuss the relationship between FGA and aneuploidy (related but different).
Based on this problem, the author added the comparison between the text and FGA, which is figure1F of the original text.
2: It seems that the benefit of using a 20% cutoff for aneuploidy score is more obvious.
Based on this problem, the author added the analysis of the original figure2A.
3: Is it possible that most of the effects are due to specific chromosomal changes (e.g. 9p21 deletion) rather than aneuploidy.
Based on this problem, the author added the chromosome arm amplification deletion analysis we mentioned above.
4: Can the authors present a clinically relevant case? The true value of TMB itself is actually not very large (rarely used clinically), and the effect of aneuploidy seems to be even smaller. While this biological question is interesting, I don’t believe it will affect clinical practice.
This question is quite interesting. For this kind of retrospective analysis, it is difficult for the author to really provide an example for the review to guide patients’ immunotherapy according to the aneuploidy score.
In the reply, the author first emphasized through a newly published literature (PMID 35764740) that the biggest problem in the clinical application of TMB should be to study which patients with low TMB have abnormal genome-wide structure of tumors related to the efficacy of ICI, and then put forward their own The research just meets the actual clinical needs that everyone is most concerned about.
At the same time, the author again emphasized the 2-year OS difference between different tumors under the comparison of TMB and aneuploidy groups, and then emphasized that compared with the TMB group, the aneuploidy score had a stronger impact on the prognosis of breast and kidney cancer patients. big. Finally, I added that based on this result, it is believed that the huge difference in OS of aneuploidy is worthy of further prospective verification in combination with TMB.
The author of this article : bear who thinks about problems
Copyright statement : Unless otherwise stated, all articles on this blog are licensed under the Creative Commons Attribution-Non-Commercial Use-No Derivatives 4.0 International License Agreement (CC BY-NC-ND 4.0) .
If you are interested in this article, please subscribe to my “Xiong Yan Xiong Yu” member newsletter via email or WeChat. I will share with you the latest research progress in the field of biomedicine and what I think and learn. , click this link to subscribe for free.
This article is reproduced from: https://kaopubear.top/blog/2022-12-02-tumor-aneuploidy-predicts-ici-survival/
This site is only for collection, and the copyright belongs to the original author.